11 Countries Have Reported Polio Cases During 2019


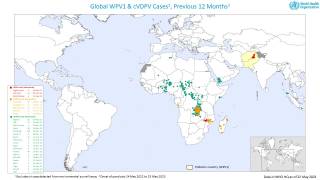
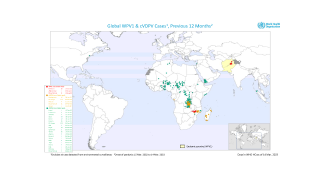
The World Health Organization (WHO) published an update regarding the ongoing expansion of poliovirus cases around the world.
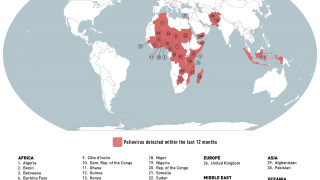
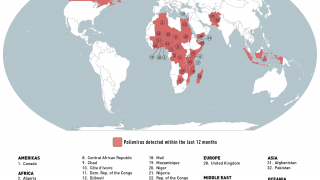
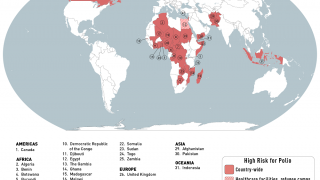
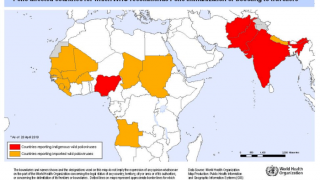
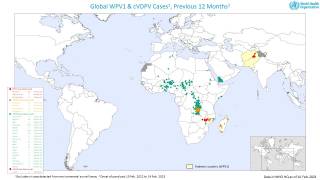
As of July 31, 2019, the WHO reported 11 countries have confirmed circulating vaccine-derived poliovirus type 2 (cVDPV2) outbreaks.
Additionally, the WHO assesses the risk of international spread and/or the emergence of cVDPV2 across Africa to be ‘high’ due to suboptimal immunity of population, ongoing population movement, and increasing mucosal immunity gaps to type 2 poliovirus.
Furthermore, it is important that all countries, in particular, those with frequent travel and contacts with polio-affected countries and areas, strengthen surveillance for Acute Flaccid Paralysis (AFP) cases in order to rapidly detect any new virus importation and to facilitate a rapid response.
Excerpts from this new WHO report for the African and Eastern Mediterranean regions are below:
Lake Chad Basin (LCB) sub-region
- In the Lake Chad Basin sub-region, which includes Niger, Cameroon, and Nigeria, multiple cVDPV2 outbreaks continue to spread.
- In Niger, an outbreak of cVDPV2 was reported in the health districts of Magaria and Tanout in the Zinder region. As of 22 July 2019, a total of 22 cVDPV2 have been reported in the country since the outbreak began in July 2018 from Magaria, Tanout, Dungass, and Bosso. Genetic sequencing of the viruses indicated that they were linked to the outbreak in Borno state, Nigeria.
- As an extension of the outbreaks in the LCB, a cVDPV2 was isolated from an environmental sample collected from the Koblimagu site in Tamale Metropolis in Ghana, on 11 July 2019. Genetic sequencing of the virus indicated that it was linked to the outbreaks in the Kwara state of Nigeria.
Nigeria
- In Nigeria, 17 states have been affected including Adamawa, Bauchi, Borno, Gombe, Jigawa, Kaduna, Kano, Katsina, Kwara, Lagos, Niger, Ogun, Osun, Sokoto, Taraba, Yobe and Zamfara states. The viruses isolated from most of the states are genetically linked to the outbreak in Jigawa that was reported on 13 October 2018, though separate cVDPV2 were detected in Borno and Sokoto states.
- As of 22 July 2019, 50 samples from the environment have tested positive for cVDPV2 while the virus has been isolated from the stool samples of 23 children who presented with acute flaccid paralysis (AFP) or in healthy community contacts.
Cameroon
- On 16 May 2019, the Centre Pasteur of Cameroon isolated a cVDPV2 from an environmental sample collected from the Mada District Hospital site on 20 April 2019 in the Far North region of the country. Genetic sequencing of the isolates also confirmed that it was linked to the ongoing outbreak in Borno state, Nigeria.
The Democratic Republic of the Congo
- From January 2018 to 5 July 2019, a total of 31 cases of cVDPV2 have been reported from seven provinces across the Democratic Republic of the Congo, namely; Mongala (11), Haut Katanga (4), Kasai (4), Haut-Lomami (5), Sankuru (4), Tanganyika (2), and Ituri (1).
- The latest case was reported from the Kamonia health zone in Kasai who experienced the onset of symptoms on 28 May 2019. The 26 cases reported since 2018 have been associated to seven genetically-distinct cVDPV2 strains affecting the seven provinces, with Kasai and Haut-Lomami being affected by two distinct cVDPV2 strains each.
- In Kasai province, two new genetically-linked viruses, with six nucleotide changes from Sabin 2 for both, were isolated from two separate AFP cases with onset of paralysis on 8 and 21 April 2019. Kasai had already been participating in mOPV2 outbreak campaigns, as it had already been affected by a separate cVDPV2 outbreak.
Angola
- In Angola, two genetically-distinct outbreaks of cVDPV2 have been detected in Luanda Norte and Huila provinces in 2019.
- The first case of cVDPV2, with ten nucleotides changes from Sabin 2, was isolated from an AFP case with onset of paralysis on 22 March 2018. The case was reported during the week 23 (week ending 9 June 2019) from Lunda Norte province, bordering the Democratic Republic of the Congo.
The Central African Republic
- In the Central African Republic (CAR), several genetically-distinct VDPV2s have emerged and a cVDPV2 has been confirmed. VDPV2 was isolated from an AFP case with onset of paralysis on 4 May 2019, from Bambari district Region Sanitaire 4 (RS4), as well as from a healthy community contact.
- The isolated virus has 10 nucleotide changes from Sabin 2 and is not known to VDPV2s circulating elsewhere in the region, suggesting it is a new emergence.
- Additionally, poliovirus type 2 has been isolated from five healthy close contacts of the case, and final sequencing of these viruses are pending.
- Separately, a VDPV2 was isolated from an AFP case from RS7 province, with the onset of paralysis on 6 May, with 6 nucleotide changes from Sabin 2 and unrelated to the VDPV2 confirmed in RS4. IPV coverage in the CAR was 47% for the country in 2018.
Ethiopia / Somalia / Kenya - Horn of Africa
- A cVDPV2 outbreak in the Horn of Africa has been detected in Somali province, Ethiopia. The virus was isolated from an AFP case with onset of paralysis on 20 May 2019. Genetic sequencing confirms that the isolated virus is linked to an ongoing cVDPV2 outbreak detected in the Horn of Africa in 2018, with cases reported in Somalia as well as from an environmental sample in Kenya.
- Since detection of the cVDPVs in the Horn of Africa in 2018, Ethiopia had declared this outbreak – together with the Ministries of Health of Kenya and Somalia – to be a regional public health emergency and has been participating in regional outbreak response.
- Given cross-border population movements across the Horn of Africa specifically between Somalia, Kenya, and Ethiopia, as well as suboptimal subnational immunity and surveillance gaps, the Horn of Africa, is considered at high risk of further transmission of this cVDPV2.
The detection of cVDPV2s underscores the importance of maintaining high routine vaccination coverage everywhere to minimize the risk and consequences of any poliovirus circulation.
In the USA, polio has been eliminated thanks to widespread polio vaccinations. Since 1979, no new cases of polio have originated in the United States, says the US Centers for Disease Control and Prevention (CDC).
Polio is a highly infectious disease caused by a virus. It invades the nervous system and can cause total paralysis in a matter of hours. Among those paralyzed, 5 to 10 percent die when their breathing muscles become immobilized.
Of the 3 strains of wild poliovirus (type 1, type 2, and type 3), no case of wild poliovirus type 3 has been found since the last reported case in Nigeria in November 2012.
The WHO’s International Travel and Health recommend that all travelers to polio-affected areas be fully vaccinated against polio. Residents (and visitors for more than 4 weeks) from infected areas should receive an additional dose of OPV or inactivated polio vaccine (IPV) within 4 weeks to 12 months of travel.
Only the IPV has been used in the United States since 2000, but the OPV is still used throughout much of the world.
Pre-trip, polio vaccine counseling appointments can be scheduled with a local travel pharmacy at Vax-Before-Travel.
Polio vaccines, like any medicine, can have side effects. You are encouraged to report polio vaccine side effects to a healthcare provider or the CDC.
Our Trust Standards: Medical Advisory Committee
-
Fact checked by Robert Carlson, MD